It's time for a new paradigm.
From the 16th century to the 19th, scurvy killed around 2 million sailors, more than warfare, shipwrecks and syphilis combined. It was an ugly, smelly death, too, beginning with rattling teeth and ending with a body so rotted out from the inside that its victims could literally be startled to death by a loud noise. Just as horrifying as the disease itself, though, is that for most of those 300 years, medical experts knew how to prevent it and simply failed to.
In the 1600s, some sea captains distributed lemons, limes and oranges to sailors, driven by the belief that a daily dose of citrus fruit would stave off scurvy's progress. The British Navy, wary of the cost of expanding the treatment, turned to malt wort, a mashed and cooked byproduct of barley which had the advantage of being cheaper but the disadvantage of doing nothing whatsoever to cure scurvy. In 1747, a British doctor named James Lind conducted an experiment where he gave one group of sailors citrus slices and the others vinegar or seawater or cider. The results couldn't have been clearer. The crewmen who ate fruit improved so quickly that they were able to help care for the others as they languished. Lind published his findings, but died before anyone got around to implementing them nearly 50 years later.
This kind of myopia repeats throughout history. Seat belts were invented long before the automobile but weren't mandatory in cars until the 1960s. The first confirmed death from asbestos exposure was recorded in 1906, but the U.S. didn't start banning the chemical until 1973. Every discovery in public health, no matter how significant, must compete with the traditions, assumptions and financial incentives of the society implementing it.
Which brings us to one of the largest gaps between science and practice in our own time. Years from now, we will look back in horror at the counterproductive ways we addressed the obesity epidemic and the barbaric ways we treated fat people—long after we knew there was a better path.
I have never written a story where so many of my sources cried during interviews, where they shook with anger describing their interactions with doctors and strangers and their own families.About 40 years ago, Americans started getting much larger. According to the Centers for Disease Control and Prevention, nearly 80 percent of adultsand about one-third of children now meet the clinical definition of overweight or obese. More Americans live with "extreme obesity" than with breast cancer, Parkinson's, Alzheimer's and HIV put together.
And the medical community's primary response to this shift has been to blame fat people for being fat. Obesity, we are told, is a personal failing that strains our health care system, shrinks our GDP and saps our military strength. It is also an excuse to bully fat people in one sentence and then inform them in the next that you are doing it for their own good. That's why the fear of becoming fat, or staying that way, drives Americans to spend more on dieting every year than we spend on video games or movies. Forty-five percent of adults say they're preoccupied with their weight some or all of the time—an 11-point rise since 1990. Nearly half of 3- to 6- year old girls say they worry about being fat.
The emotional costs are incalculable. I have never written a story where so many of my sources cried during interviews, where they double- and triple-checked that I would not reveal their names, where they shook with anger describing their interactions with doctors and strangers and their own families. One remembered kids singing "Baby Beluga" as she boarded the school bus, another said she has tried diets so extreme she has passed out and yet another described the elaborate measures he takes to keep his spouse from seeing him naked in the light. A medical technician I'll call Sam (he asked me to change his name so his wife wouldn't find out he spoke to me) said that one glimpse of himself in a mirror can destroy his mood for days. "I have this sense I'm fat and I shouldn't be," he says. "It feels like the worst kind of weakness."
My interest in this issue is slightly more than journalistic. Growing up, my mother's weight was the uncredited co-star of every family drama, the obvious, unspoken reason why she never got out of the car when she picked me up from school, why she disappeared from the family photo album for years at a time, why she spent hours making meatloaf then sat beside us eating a bowl of carrots. Last year, for the first time, we talked about her weight in detail. When I asked if she was ever bullied, she recalled some guy calling her a "fat slob" as she biked past him years ago. "But that was rare," she says. "The bigger way my weight affected my life was that I waited to do things because I thought fat people couldn't do them." She got her master's degree at 38, her Ph.D. at 55. "I avoided so many activities where I thought my weight would discredit me."
Chances of a woman classified as obese achieving a "normal" weight:.008%SOURCE: AMERICAN JOURNAL OF PUBLIC HEALTH, 2015But my mother's story, like Sam's, like everyone's, didn't have to turn out like this. For 60 years, doctors and researchers have known two things that could have improved, or even saved, millions of lives. The first is that diets do not work. Not just paleo or Atkins or Weight Watchers or Goop, but all diets. Since 1959, research has shown that 95 to 98 percent of attempts to lose weight fail and that two-thirds of dieters gain back more than they lost. The reasons are biological and irreversible. As early as 1969, research showed that losing just 3 percent of your body weight resulted in a 17 percent slowdown in your metabolism—a body-wide starvation response that blasts you with hunger hormones and drops your internal temperature until you rise back to your highest weight. Keeping weight off means fighting your body's energy-regulation system and battling hunger all day, every day, for the rest of your life.
The second big lesson the medical establishment has learned and rejected over and over again is that weight and health are not perfect synonyms. Yes, nearly every population-level study finds that fat people have worse cardiovascular health than thin people. But individuals are not averages: Studies have found that anywhere from one-third to three-quarters of people classified as obese are metabolically healthy. They show no signs of elevated blood pressure, insulin resistance or high cholesterol. Meanwhile, about a quarter of non-overweight people are what epidemiologists call "the lean unhealthy." A 2016 study that followed participants for an average of 19 years found that unfit skinny people were twice as likely to get diabetes as fit fat people. Habits, no matter your size, are what really matter. Dozens of indicators, from vegetable consumption to regular exercise to grip strength, provide a better snapshot of someone's health than looking at her from across a room.
The terrible irony is that for 60 years, we've approached the obesity epidemic like a fad dieter: If we just try the exact same thing one more time, we'll get a different result. And so it's time for a paradigm shift. We're not going to become a skinnier country. But we still have a chance to become a healthier one.

This is Corissa Enneking at her lightest: She wakes up, showers and smokes a cigarette to keep her appetite down. She drives to her job at a furniture store, she stands in four-inch heels all day, she eats a cup of yogurt alone in her car on her lunch break. After work, lightheaded, her feet throbbing, she counts out three Ritz crackers, eats them at her kitchen counter and writes down the calories in her food journal.
Or not. Some days she comes home and goes straight to bed, exhausted and dizzy from hunger, shivering in the Kansas heat. She rouses herself around dinnertime and drinks some orange juice or eats half a granola bar. Occasionally she'll just sleep through the night, waking up the next day to start all over again.
The last time she lived like this, a few years ago, her mother marched her to the hospital. "My daughter is sick," she told the doctor. "She's not eating." He looked Enneking up and down. Despite six months of starvation, she was still wearing plus sizes, still couldn't shop at J. Crew, still got unsolicited diet advice from colleagues and customers.
Enneking told the doctor that she used to be larger, that she'd lost some weight the same way she had lost it three or four times before—seeing how far she could get through the day without eating, trading solids for liquids, food for sleep. She was hungry all the time, but she was learning to like it. When she did eat, she got panic attacks. Her boss was starting to notice her erratic behavior.
"Well, whatever you're doing now," the doctor said, "it's working." He urged her to keep it up and assured her that once she got small enough, her body would start to process food differently. She could add a few hundred calories to her diet. Her period would come back. She would stay small, but without as much effort.
"If you looked at anything other than my weight," Enneking says now, "I had an eating disorder. And my doctor was congratulating me."
Ask almost any fat person about her interactions with the health care system and you will hear a story, sometimes three, the same as Enneking's: rolled eyes, skeptical questions, treatments denied or delayed or revoked. Doctors are supposed to be trusted authorities, a patient's primary gateway to healing. But for fat people, they are a source of unique and persistent trauma. No matter what you go in for or how much you're hurting, the first thing you will be told is that it would all get better if you could just put down the Cheetos.
Emily went to a gynecological surgeon to have an ovarian cyst removed. The physician pointed out her body fat on the MRI, then said, "Look at that skinny woman in there trying to get out."This phenomenon is not merely anecdotal. Doctors have shorterappointments with fat patients and show less emotional rapport in the minutes they do have. Negative words—"noncompliant," "overindulgent," "weak willed"—pop up in their medical histories with higher frequency. In one study, researchers presented doctors with case histories of patients suffering from migraines. With everything else being equal, the doctors reported that the patients who were also classified as fat had a worse attitude and were less likely to follow their advice. And that's when they see fat patients at all: In 2011, the Sun-Sentinel polled OB-GYNs in South Florida and discovered that 14 percent had barred all new patients weighing more than 200 pounds.
Some of these doctors are simply applying the same presumptions as the society around them. An anesthesiologist on the West Coast tells me that as soon as a larger patient goes under, the surgeons start trading "high school insults" about her body over the operating table. Janice O'Keefe, a former nurse in Boston, tells me a doctor once looked at her, paused, then asked, "How could you do this to yourself?" Emily, a counselor in Eastern Washington, went to a gynecological surgeon to have an ovarian cyst removed. The physician pointed out her body fat on the MRI, then said, "Look at that skinny woman in there trying to get out."
"I was worried I had cancer," Emily says, "and she was turning it into a teachable moment about my weight."
Other physicians sincerely believe that shaming fat people is the best way to motivate them to lose weight. "It's the last area of medicine where we prescribe tough love," says Mayo Clinic researcher Sean Phelan.
In a 2013 journal article, bioethicist Daniel Callahan argued for morestigma against fat people. "People don't realize that they are obese or if they do realize it, it's not enough to stir them to do anything about it," he tells me. Shame helped him kick his cigarette habit, he argues, so it should work for obesity too.
This belief is cartoonishly out of step with a generation of research into obesity and human behavior. As one of the (many) stigma researchers who responded to Callahan's article pointed out, shaming smokers and drug users with D.A.R.E.-style "just say no" messages may have actually increased substance abuse by making addicts less likely to bring up their habit with their doctors and family members.
Plus, rather obviously, smoking is a behavior; being fat is not. Jody Dushay, an endocrinologist and obesity specialist at Beth Israel Deaconess Medical Center in Boston, says most of her patients have tried dozens of diets and have lost and regained hundreds of pounds before they come to her. Telling them to try again, but in harsher terms, only sets them up to fail and then blame themselves.
89%of obese adults have been bullied by their romantic partnersSOURCE: UNIVERSITY OF CONNECTICUT, 2017Not all physicians set out to denigrate their fat patients, of course; some of them do damage because of subtler, more unconscious biases. Most doctors, for example, are fit—"If you go to an obesity conference, good luck trying to get a treadmill at 5 a.m.," Dushay says—and have spent more than a decade of their lives in the high-stakes, high-stress bubble of medical schools. According to several studies, thin doctors are more confident in their recommendations, expect their patients to lose more weight and are more likely to think dieting is easy. Sarah (not her real name), a tech CEO in New England, once told her doctor that she was having trouble eating less throughout the day. "Look at me," her doctor said. "I had one egg for breakfast and I feel fine."
Then there are the glaring cultural differences. Kenneth Resnicow, a consultant who trains physicians to build rapport with their patients, says white, wealthy, skinny doctors will often try to bond with their low-income patients by telling them, "I know what it's like not to have time to cook." Their patients, who might be single mothers with three kids and two jobs, immediately think "No, you don't," and the relationship is irretrievably soured.
When Joy Cox, an academic in New Jersey, was 16, she went to the hospital with stomach pains. The doctor didn't diagnose her dangerously inflamed bile duct, but he did, out of nowhere, suggest that she'd get better if she stopped eating so much fried chicken. "He managed to denigrate my fatness and my blackness in the same sentence," she says.

Many of the financial and administrative structures doctors work within help reinforce this bad behavior. The problem starts in medical school, where, according to a 2015 survey, students receive an average of just 19 hours of nutrition education over four years of instruction—five hours fewer than they got in 2006. Then the trouble compounds once doctors get into daily practice. Primary care physicians only get 15 minutes for each appointment, barely enough time to ask patients what they ate today, much less during all the years leading up to it. And a more empathic approach to treatment simply doesn't pay: While procedures like blood tests and CT scans command reimbursement rates from hundreds to thousands of dollars, doctors receive as little as $24 to provide a session of diet and nutrition counseling.
Lesley Williams, a family medicine doctor in Phoenix, tells me she gets an alert from her electronic health records software every time she's about to see a patient who is above the "overweight" threshold. The reason for this is that physicians are often required, in writing, to prove to hospital administrators and insurance providers that they have brought up their patient's weight and formulated a plan to bring it down—regardless of whether that patient came in with arthritis or a broken arm or a bad sunburn. Failing to do that could result in poor performance reviews, low ratings from insurance companies or being denied reimbursement if they refer patients to specialized care.
Another issue, says Kimberly Gudzune, an obesity specialist at Johns Hopkins, is that many doctors, no matter their specialty, think weight falls under their authority. Gudzune often spends months working with patients to set realistic goals—playing with their grandkids longer, going off a cholesterol medication—only to have other doctors threaten it all. One of her patients was making significant progress until she went to a cardiologist who told her to lose 100 pounds. "All of a sudden she goes back to feeling like a failure and we have to start over," Gudzune says. "Or maybe she just never comes back at all."
60%of the calories Americans consume come from "ultra-processed foods"SOURCE: BRITISH MEDICAL JOURNAL, 2016And so, working within a system that neither trains nor encourages them to meaningfully engage with their higher-weight patients, doctors fall back on recommending fad diets and delivering bland motivational platitudes. Ron Kirk, an electrician in Boston, says that for years, his doctor's first resort was to put him on some diet he couldn't maintain for more than a few weeks. "They told me lettuce was a 'free' food," he says—and he'd find himself carving up a head of romaine for dinner.
In a study that recorded 461 interactions with doctors, only 13 percent of patients got any specific plan for diet or exercise and only 5 percent got help arranging a follow-up visit. "It can be stressful when [patients] start asking a lot of specific questions" about diet and weight loss, one doctor told researchers in 2012. "I don't feel like I have the time to sit there and give them private counseling on basics. I say, 'Here's some websites, look at this.'" A 2016 survey found that nearly twice as many higher-weight Americans have tried meal-replacement diets—the kind most likely to fail—than have ever received counseling from a dietician.
"It borders on medical malpractice," says Andrew (not his real name), a consultant and musician who has been large his whole life. A few years ago, on a routine visit, Andrew's doctor weighed him, announced that he was "dangerously overweight" and told him to diet and exercise, offering no further specifics. Should he go on a low-fat diet? Low-carb? Become a vegetarian? Should he do Crossfit? Yoga? Should he buy a fucking ThighMaster?
"She didn't even ask me what I was already doing for exercise," he says. "At the time, I was training for serious winter mountaineering trips, hiking every weekend and going to the gym four times a week. Instead of a conversation, I got a sound bite. It felt like shaming me was the entire purpose."
All of this makes higher-weight patients more likely to avoid doctors. Three separate studies have found that fat women are more likely to die from breast and cervical cancers than non-fat women, a result partially attributed to their reluctance to see doctors and get screenings. Erin Harrop, a researcher at the University of Washington, studies higher-weight women with anorexia, who, contrary to the size-zero stereotype of most media depictions, are twice as likely to report vomiting, using laxatives and abusing diet pills. Thin women, Harrop discovered, take around three years to get into treatment, while her participants spent an average of 13 and a half years waiting for their disorders to be addressed.
"A lot of my job is helping people heal from the trauma of interacting with the medical system," says Ginette Lenham, a counselor who specializes in obesity. The rest of it, she says, is helping them heal from the trauma of interacting with everyone else.

If Sonya ever forgets that she is fat, the world will remind her. She has stopped taking the bus, she tells me, because she can sense the aggravation of the passengers squeezing past her. Sarah, the tech CEO, tenses up when anyone brings bagels to a work meeting. If she reaches for one, are her employees thinking, "There goes the fat boss"? If she doesn't, are they silently congratulating her for showing some restraint?
Emily says it's the do-gooders who get to her, the women who stop her on the street and tell her how brave she is for wearing a sleeveless dress on a 95-degree day. Sam, the medical technician, avoids the subject of weight altogether. "Men aren't supposed to think about this stuff—and I think about it constantly," he admits. "So I never let myself talk about it. Which is weird because it's the most visible thing about me."
Again and again I hear stories of how the pressure to be a "good fatty" in public builds up and explodes. Jessica has four kids. Every week is a birthday party or family reunion or swimming pool social, another opportunity to stand around platters of spare ribs and dinner rolls with her fellow moms.
"Your conscious mind is busy the whole day with how many calories is in everything, what you can eat and who's watching," she says. After a few intrusive comments over the years—should you be eating that?—she has learned to be careful, to perform the role of the impeccable fat person. She nibbles on cherry tomatoes, drinks tap water, stays on her feet, ignores the dessert end of the buffet.
Then, as the gathering winds down, Jessica and the other parents divvy up the leftovers. She wraps up burgers or pasta salad or birthday cake, drives her children home and waits for the moment when they are finally in bed. Then, when she's alone, she eats all the leftovers by herself, in the dark.
"It's always hidden," she says. "I buy a package of ice cream, then eat it all. Then I have to go to the store to buy it again. For a week my family thinks there's a thing of ice cream in the fridge—but it's actually five different ones."
Ratio of soda and candy ads seen by black children compared to white children:2:1SOURCE: UCONN RUDD CENTER FOR FOOD POLICY AND OBESITY, 2015This is how fat-shaming works: It is visible and invisible, public and private, hidden and everywhere at the same time. Research consistently finds that larger Americans (especially larger women) earn lower salariesand are less likely to be hired and promoted. In a 2017 survey, 500 hiring managers were given a photo of an overweight female applicant. Twenty-one percent of them described her as unprofessional despite having no other information about her. What's worse, only a few cities and one state (nice work, Michigan) officially prohibit workplace discrimination on the basis of weight.
Paradoxically, as the number of larger Americans has risen, the biases against them have become more severe. More than 40 percent of Americans classified as obese now say they experience stigma on a daily basis, a rate far higher than any other minority group. And this does terrible things to their bodies. According to a 2015 study, fat people who feel discriminated against have shorter life expectancies than fat people who don't. "These findings suggest the possibility that the stigma associated with being overweight," the study concluded, "is more harmful than actually being overweight."
And, in a cruel twist, one effect of weight bias is that it actually makes you eat more. The stress hormone cortisol—the one evolution designed to kick in when you're being chased by a tiger or, it turns out, rejected for your looks—increases appetite, reduces the will to exercise and even improves the taste of food. Sam, echoing so many of the other people I spoke with, says that he drove straight to Jack in the Box last year after someone yelled, "Eat less!" at him across a parking lot.

There's a grim caveman logic to our nastiness toward fat people. "We're attuned to bodies that look different," says Janet Tomiyama, a stigma researcher at UCLA. "In our evolutionary past, that might have meant disease risk and been seen as a threat to your tribe." These biological breadcrumbs help explain why stigma begins so early. Kids as young as 3 describe their larger classmates with words like "mean," "stupid" and "lazy."
And yet, despite weight being the number one reason children are bullied at school, America's institutions of public health continue to pursue policies perfectly designed to inflame the cruelty. TV and billboard campaigns still use slogans like "Too much screen time, too much kid" and "Being fat takes the fun out of being a kid." Cat Pausé, a researcher at Massey University in New Zealand, spent months looking for a single public health campaign, worldwide, that attempted to reduce stigma against fat people and came up empty. In an incendiary case of good intentions gone bad, about a dozen states now send children home with "BMI report cards," an intervention unlikely to have any effect on their weight but almost certain to increase bullying from the people closest to them.
This is not an abstract concern: Surveys of higher-weight adults find that their worst experiences of discrimination come from their own families. Erika, a health educator in Washington, can still recite the word her father used to describe her: "husky." Her grandfather preferred "stocky." Her mother never said anything about Erika's body, but she didn't have to. She obsessed over her own, calling herself "enormous" despite being two sizes smaller than her daughter. By the time Erika was 11, she was sneaking into the woods behind her house and vomiting into the creek whenever social occasions made starving herself impossible.
And the abuse from loved ones continues well into adulthood. A 2017 survey found that 89 percent of obese adults had been bullied by their romantic partners. Emily, the counselor, says she spent her teens and 20s "sleeping with guys I wasn't interested in because they wanted to sleep with me." In her head, a guy being into her was a rare and depletable resource she couldn't afford to waste: "I was desperate for men to give me attention. Sex was a good way to do that."
Eventually, she ended up with someone abusive. He told her during sex that her body was beautiful and then, in the daylight, that it was revolting. "Whenever I tried to leave him, he would say, 'Where are you gonna find someone who will put up with your disgusting body?'" she remembers.
Emily finally managed to get away from him, but she is aware that her love life will always be fraught. The guy she's dating now is thin—"think Tony Hawk," she says—and she notices the looks they get when they hold hands in public. "That never used to happen when I dated fat dudes," she says. "Thin men are not allowed to be attracted to fat women."
The effects of weight bias get worse when they're layered on top of other types of discrimination. A 2012 study found that African-American women are more likely to become depressed after internalizing weight stigma than white women. Hispanic and black teenagers also have significantly higher rates of bulimia. And, in a remarkable finding, rich people of color have higher rates of cardiovascular disease than poor people of color—the opposite of what happens with white people. One explanation is that navigating increasingly white spaces, and increasingly higher stakes, exerts stress on racial minorities that, over time, makes them more susceptible to heart problems.
But perhaps the most unique aspect of weight stigma is how it isolates its victims from one another. For most minority groups, discrimination contributes to a sense of belongingness, a community in opposition to a majority. Gay people like other gay people; Mormons root for other Mormons. Surveys of higher-weight people, however, reveal that they hold many of the same biases as the people discriminating against them. In a 2005 study, the words obese participants used to classify other obese people included gluttonous, unclean and sluggish.
Andrea, a retired nurse in Boston, has been on commercial diets since she was 10 years old. She knows how hard it is to slim down, knows what women larger than her are going through, but she still struggles not to pass judgment when she sees them in public. "I think, 'How did they let it happen?'" she says. "It's more like fear. Because if I let myself go, I'll be that big too."
Her position is all-too understandable. As young as 9 or 10, I knew that coming out of the closet is what gay people do, even if it took me another decade to actually do it. Fat people, though, never get a moment of declaring their identity, of marking themselves as part of a distinct group. They still live in a society that believes weight is temporary, that losing it is urgent and achievable, that being comfortable in their bodies is merely "glorifying obesity." This limbo, this lie, is why it's so hard for fat people to discover one another or even themselves. "No one believes our It Gets Better story," says Tigress Osborn, the director of community outreach for the National Association to Advance Fat Acceptance. "You can't claim an identity if everyone around you is saying it doesn't or shouldn't exist."
Harrop, the eating disorders researcher, realized several years ago that her university had clubs for trans students, immigrant students, Republican students, but none for fat students. So she started one—and it has been a resounding, unmitigated failure. Only a handful of fat people have ever showed up; most of the time, thin folks sit around brainstorming about how to be better allies.
I ask Harrop why she thinks the group has been such a bust. It's simple, she says: "Fat people grow up in the same fat-hating culture that non-fat people do."

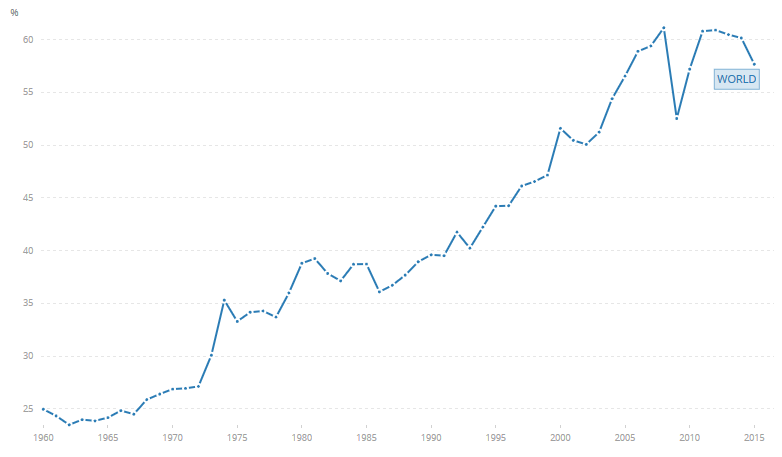
Since 1980, the obesity rate has doubled in 73 countries and increased in 113 others. And in all that time, no nation has reduced its obesity rate. Not one.
The problem is that in America, like everywhere else, our institutions of public health have become so obsessed with body weight that they have overlooked what is really killing us: our food supply. Diet is the leading cause of death in the United States, responsible for more than five times the fatalities of gun violence and car accidents combined. But it's not how much we're eating—Americans actually consume fewer calories now than we did in 2003. It's what we're eating.
For more than a decade now, researchers have found that the quality of our food affects disease risk independently of its effect on weight. Fructose, for example, appears to damage insulin sensitivity and liver function more than other sweeteners with the same number of calories. People who eat nuts four times a week have 12 percent lower diabetes incidence and a 13 percent lower mortality rate regardless of their weight. All of our biological systems for regulating energy, hunger and satiety get thrown off by eating foods that are high in sugar, low in fiber and injected with additives. And which now, shockingly, make up 60 percent of the calories we eat.
Draining this poison from our trillion-dollar food system is not going to happen quickly or easily. Every link in the chain, from factory farms to school lunches, is dominated by a Mars or a Monsanto or a McDonald's, each working tirelessly to lower its costs and raise its profits. But that's still no reason to despair. There's a lot we can do right now to improve fat people's lives—to shift our focus for the first time from weight to health and from shame to support.
The place to start is at the doctor's office. The central failure of the medical system when it comes to obesity is that it treats every patient exactly the same: If you're fat, lose some weight. If you're skinny, keep up the good work. Stephanie Sogg, a psychologist at the Mass General Weight Center, tells me she has clients who start eating compulsively after a sexual assault, others who starve themselves all day before bingeing on the commute home and others who eat 1,000 calories a day, work out five times a week and still insist that they're fat because they "have no willpower."
Acknowledging the infinite complexity of each person's relationship to food, exercise and body image is at the center of her treatment, not a footnote to it. "Eighty percent of my patients cry in the first appointment," Sogg says. "For something as emotional as weight, you have to listen for a long time before you give any advice. Telling someone, 'Lay off the cheeseburgers' is never going to work if you don't know what those cheeseburgers are doing for them."
4%of all agricultural subsidies go to fruits and vegetablesSOURCE: ENVIRONMENTAL WORKING GROUP, 2014-16The medical benefits of this approach—being nicer to her patients than they are to themselves, is how Sogg describes it—are unimpeachable. In 2017, the U.S. Preventive Services Task Force, the expert panel that decides which treatments should be offered for free under Obamacare, found that the decisive factor in obesity care was not the diet patients went on, but how much attention and support they received while they were on it. Participants who got more than 12 sessions with a dietician saw significant reductions in their rates of prediabetes and cardiovascular risk. Those who got less personalized care showed almost no improvement at all.
Still, despite the Task Force's explicit recommendation of "intensive, multicomponent behavioral counseling" for higher-weight patients, the vast majority of insurance companies and state health care programs define this term to mean just a session or two—exactly the superficial approach that years of research says won't work. "Health plans refuse to treat this as anything other than a personal problem," says Chris Gallagher, a policy consultant at the Obesity Action Coalition.
The same scurvy-ish negligence shows up at every level of government. From marketing rules to antitrust regulations to international trade agreements, U.S. policy has created a food system that excels at producing flour, sugar and oil but struggles to deliver nutrients at anywhere near the same scale. The United States spends $1.5 billion on nutrition research every year compared to around $60 billion on drug research. Just 4 percent of agricultural subsidies go to fruits and vegetables. No wonder that the healthiest foods can cost up to eight times more, calorie for calorie, than the unhealthiest—or that the gap gets wider every year.
It's the same with exercise. The cardiovascular risks of sedentary lifestyles, suburban sprawl and long commutes are well-documented. But rather than help mitigate these risks—and their disproportionate impact on the poor—our institutions have exacerbated them. Only 13 percent of American children walk or bike to school; once they arrive, less than a third of them will take part in a daily gym class. Among adults, the number of workers commuting more than 90 minutes each way grew by more than 15 percent from 2005 to 2016, a predictable outgrowth of America's underinvestment in public transportation and over-investment in freeways, parking and strip malls. For 40 years, as politicians have told us to eat more vegetables and take the stairs instead of the elevator, they have presided over a country where daily exercise has become a luxury and eating well has become extortionate.

The good news is that the best ideas for reversing these trends have already been tested. Many "failed" obesity interventions are, in fact, successful eat-healthier-and-exercise-more interventions. A review of 44 international studies found that school-based activity programs didn't affect kids' weight, but improved their athletic ability, tripled the amount of time they spent exercising and reduced their daily TV consumption by up to an hour. Another survey showed that two years of getting kids to exercise and eat better didn't noticeably affect their size but did improve their math scores—an effect that was greater for black kids than white kids.
You see this in so much of the research: The most effective health interventions aren't actually health interventions—they are policies that ease the hardship of poverty and free up time for movement and play and parenting. Developing countries with higher wages for women have lower obesity rates, and lives are transformed when healthy food is made cheaper. A pilot program in Massachusetts that gave food stamp recipients an extra 30 cents for every $1 they spent on healthy food increased fruit and vegetable consumption by 26 percent. Policies like this are unlikely to affect our weight. They are almost certain, however, to significantly improve our health.
Which brings us to the most hard-wired problem of all: Our shitty attitudes toward fat people. According to Patrick Corrigan, the editor of the journal Stigma and Health, even the most well-intentioned efforts to reduce stigma break down in the face of reality. In one study, researchers told 10- to 12-year-olds all the genetic and medical factors that contribute to obesity. Afterward, the kids could recite back the message they received—fat kids didn't get that way by choice—but they still had the same negative attitudes about the bigger kids sitting next to them. A similar approach with fifth- and sixth-graders actually increased their intention of bullying their fat classmates. Celebrity representation, meanwhile, can result in what Corrigan calls the "Thurgood Marshall effect": Instead of updating our stereotypes (maybe fat people aren't so bad), we just see prominent minorities as isolated exceptions to them (well, he's not like those other fat people).
What does work, Corrigan says, is for fat people to make it clear to everyone they interact with that their size is nothing to apologize for. "When you pity someone, you think they're less effective, less competent, more hurt," he says. "You don't see them as capable. The only way to get rid of stigma is from power."
This has always been the great hope of the fat-acceptance movement. ("We're here, we're spheres, get used to it" was one of the slogans in the 1990s.) But this radical message has long since been co-opted by clothing brands, diet companies and soap corporations. Weight Watchers has rebranded as a "lifestyle program," but still promises that its members can shrink their way to happiness. Mainstream apparel companies market themselves as "body positive" but refuse to make clothes that fit the plus-size models on their own billboards. Social media, too, has provided a platform for positive representations of fat people and formed communities that make it easier to find each other. But it has also contributed to an anodyne, narrow, Dr. Phil-approved form of progress that celebrates the female entrepreneur who sells "fatkinis" on Instagram, while ignoring the woman who (true story) gets fired from her management position after reportedly gaining 100 pounds over three years.
"Fat activism isn't about making people feel better about themselves," Pausé says. "It's about not being denied your civil rights and not dying because a doctor misdiagnoses you."
And so, in a world that refuses to change, it is still up to every fat person, alone, to decide how to endure. Emily, the counselor in Eastern Washington, says she made a choice about three years ago to assert herself. The first time she asked for a table instead of a booth at a restaurant, she says, she was sweating, flushed, her chest heaving. It felt like saying the words—"I can't fit"—would dry up in her mouth as she said them.
But now, she says, "It's just something I do." Last month, she was at a conference and asked one of the other participants if he would trade chairs because his didn't have arms. Like most of these requests, it was no big deal. "A tall person wouldn't feel weird asking that, so why should I?" she says. Her skinny friends have started to inquire about the seating at restaurants before Emily even gets the chance.
Hearing about Emily's progress reminds me of a conversation I had with Ginette Lenham, the diet counselor. Her patients, she says, often live in the past or the future with their weight. They tell her they are waiting until they are smaller to go back to school or apply for a new job. They beg her to return them to their high school or wedding or first triathlon weight, the one that will bring back their former life.
And then Lenham must explain that these dreams are a trap. Because there is no magical cure. There is no time machine. There is only the revolutionary act of being fat and happy in a world that tells you that's impossible.
"We all have to do our best with the body that we have," she says. "And leave everyone else's alone."