Yes, TrumpCare Will Kill People
 Up until now I've been unwilling to make this claim,
Up until now I've been unwilling to make this claim,
but not because I didn't believe it.
From the beginning, it seemed like common sense to me: Losing health insurance increases your risk of dying. Uninsured people get less care, and medical care saves lives, so lack of care logically would cost lives.
Big-picture statistics backed up that intution: Other industrialized English-speaking countries provide universal healthcare, and people live longer there. (Life-expectancy-at-birth: Australia 82.15 years, Canada 81.76, United Kingdom 80.54, United States 79.68.) None of those countries is an exact duplicate of the US, but is Canada so different that its people should live two years longer, or is their healthcare system just better than ours?
I knew that people have denied this. Back in May, Republican Congressman Raul Labrador bluntly stated "Nobody dies because they don't have access to health care." During his 2012 campaign, Mitt Romney pointed to emergency rooms and asserted that everyone gets life-saving care when they really need it. "If someone has a heart attack, they don't sit in their apartment and die."
But that argument didn't impress me: Yes, the uninsured get life-saving care when they're in car accidents or having heart attacks, but a lot of the treatable things that kill people more slowly, like high blood pressure or diabetes, aren't emergencies. And while an ER might take out the tumor that's blocking your intestine and threatening to kill you in a matter of hours, it won't provide the follow-up chemotherapy or radiation that you'll need if you plan to keep on living for more than a few months.
So I kept being tempted to say that TrumpCare would kill people. Other people have: Democratic politicians like Senator Bernie Sanders and Congressman Ruben Gallego, journalists like ThinkProgress' Ian Millhiser, and doctors like Christy Duan and Andrew Goldstein. They based their claims on solid scientific studies like this one and this one.
But every time I got ready to repeat that claim, I'd google "lack of health insurance kills people" and run into articles claiming to prove the opposite or just debunk the idea that we know one way or the other. Chasing the links in those articles always led me to different scientific studies, like this one or this one.
In other words, it looked like one of those my-bubble-versus-your-bubble arguments that I try to stay out of. Liberals cherry-pick the studies they want to believe, conservatives do the same, and we all talk past each other. Yes, I think of myself as a liberal, but my true allegiance is to the reality-based community. Like Fox Mulder, I believe that the truth is out there, and I would rather find it than just go on believing whatever I'm inclined to believe anyway.
So it's been on my to-do list for months to devote some serious time to this issue, until I could feel confident that I really understood what is actually known. But given how much hard work would be involved and the possibility that I still might not arrive at a clear conclusion, that project never rose to the top of my stack. So I never boldly wrote, "TrumpCare will kill people."
Fortunately, people better equipped than myself have taken the challenge on. Benjamin Sommers, Atul Gawande, and Katherine Baicker recently published an article in The New England Journal of Medicine acknowledging the controversy and comparing the studies quoted by each side. Weighing it all, they came to this conclusion:
The body of evidence summarized here indicates that coverage expansions significantly increase patients' access to care and use of preventive care, primary care, chronic illness treatment, medications, and surgery. These increases appear to produce significant, multifaceted, and nuanced benefits to health. Some benefits may manifest in earlier detection of disease, some in better medication adherence and management of chronic conditions, and some in the psychological well-being born of knowing one can afford care when one gets sick. Such modest but cumulative changes — which one of us has called "the heroism of incremental care" — may not occur for everyone and may not happen quickly. But the evidence suggests that they do occur, and that some of these changes will ultimately help tens of thousands of people live longer lives. Conversely, the data suggest that policies that reduce coverage will produce significant harms to health, particularly among people with lower incomes and chronic conditions.
If the name Atul Gawande rings a bell, it's probably because (in addition to being a doctor and public health researcher) he's the author of popular books like Complications, Better, and Being Mortal. He also writes about health issues for The New Yorker, making him that rare researcher who's able to popularize his own work, as he did this week in "How the Senate's Health-Care Bill Threatens the Nation's Health".
To understand how the Senate Republicans' health-care bill would affect people's actual health, the first thing you have to understand is that incremental care — regular, ongoing care as opposed to heroic, emergency care — is the greatest source of value in modern medicine. There is clear evidence that people who get sufficient incremental care enjoy better prevention, earlier diagnosis and management of urgent conditions, better control of chronic illnesses, and longer life spans.
… Insurance expansions have made people more likely to get primary and preventive care, chronic-illness care, and needed medications — including cancer screenings, diabetes and blood-pressure medicines, depression treatment, and surgery for cancer before it is too late.
These improvements in care help explain why people who have health insurance are twenty-five per cent more likely to report being in good or excellent health. It also explains why they become less likely to die. Proper health care saves lives, and the magnitude of the reduction in deaths increases over time.
… Conservatives often take a narrow view of the value of health insurance: they focus on catastrophic events such as emergencies and sudden, high-cost illnesses. But the path of life isn't one of steady health punctuated by brief crises. Most of us accumulate costly, often chronic health issues as we age. These issues can often be delayed, managed, and controlled if we have good health care — and can't be if we don't.
The incremental nature of most medical interventions — the drugs I take to keep my cholesterol low might or might not prevent a heart attack in 2030 — explains why the life-saving effect of insurance is hard to find in many studies, especially ones that only examine a few years. (Sometimes a decrease in mortality is noticed, but isn't reported as a conclusion because the difference detectable within the time frame of the study isn't statistically significant yet.) For the health crises that threaten to kill you in short order, Mitt Romney is right: The ER will help you whether you are insured or not. (You may have to go bankrupt when their bill comes, but that's a different issue.)
But emergency care is far from the only way that medical care saves lives. Having watched both my parents grow old and die, I understand that many — perhaps most — deaths in this era aren't caused by a sudden crisis out of the blue. Instead, dozens of problems that are not immediately life-threatening have a way of building on each other until people get encircled by them. A sudden crisis may kill you, but only because you have gradually lost all your room to maneuver. One problem limits your mobility, another makes it hard to sleep or enjoy food, your long-time interests and activities become hard to maintain, you become feeble, and then you get depressed and stop even trying to regain your lost abilities. Whether that encirclement happens to you at 50 or at 90 depends largely on what kind of care you get.
The difficulty of measuring these kinds of outcomes and attributing them to specific causes means that precise estimates of the number of such deaths should be taken with a grain of salt. An article in Vox on Wednesday claimed that 208,500 additional people might die over the next ten years if the Senate TrumpCare bill passes. That's speculative, as the authors acknowledge. Maybe it will only be 50,000 people, maybe 400,000. Current research isn't sharp enough to be precise.
But people will die, probably quite a large number of them.
Comments
A study of what happens when you deny people ongoing medical care has already been done. https://en.wikipedia.org/wiki/Tuskegee_syphilis_experiment
While regular doctor visits are helpful, the main form of ongoing care that most people receive is in the form of medications. Medications also represent the greatest medical-related expense for most people, outside of sudden crises requiring surgery. So it shouldn't be that much of a stretch to conclude that if people can't afford medication, either because they don't have insurance, or their insurance doesn't cover it, or the copays make it unaffordable, this will have an effect on their health and will undoubtedly result in people dying who otherwise would not have.
Re: medications. My husband's high blood pressure medication costs $5 a month with health insurance, $19 a month without. But try getting a refill without a doctor's office visit. If you can afford the medication but can't afford the doctor's office visit, you're still not getting that medication.
That's a good point. I could say something similar about my cholesterol-lowering medication. Having a doctor check for side effects before reauthorizing a prescription makes sense from a medical point of view, but it is a hurdle for the uninsured.
I believe the concept of Public Health must be brought into the argument, as it affects the elite as well as the poor. It is unconvincing to discuss only individual health since some conservatives may believe the sick or handicapped weren't meant to have a long life. As an example: contagious disease. Not many people think about it anymore because it has been controlled pretty well in the USA. But, if you are a cook or a nanny who cannot afford medical care, you don't get treated. If you are sick with TB or influenza, you can pass it on…to the public, or your wealthy employer. If you are a bus driver with a distracting cancer pain, you can crash the bus…into a congressperson's limosine. Keeping the entire populace healthy is a part of keeping the individual healthy. If the elite Senators could realize they might be causing threats to themselves, perhaps they might vote differently. I would be grateful, Mr. Muder, if you could provide a better expression of this point about Public Health. Thank-you!
I agree with you. I live an apartment building whose cleaning staff is mostly Hispanic. Are they here legally? I have no idea. Whenever I hear people complain about undocumented immigrants getting medical care, I imagine the guy who cleans the banisters in the stairwells getting Ebola, but being afraid to go to a doctor.
Not sure if this was part of your reading list, but the Institute of Medicine did a fantastic series of studies in 2001-2002 about the causes & effects of uninsurance. The summary is found here:
You can download the pdf for free from the IOM's website. Although they're a little old, they are very well done, with a panel of economists and health policy experts, and I've never personally seen a more extensive or well-researched study into the health insurance market.
One interesting finding they point out: rates of insurance coverage in a community affect *everyone's* health. That is, even if you personally have health insurance, if your community has low rates of coverage, your health is affected. In hindsight, this makes perfect sense: if your community doesn't have good coverage, hospitals and doctors don't invest in providing services in your community, since they'll lose money. As a result, even for people who could afford the services, they won't be available.
This is most stark, e.g., in trauma care. Even if you're a millionaire with great insurance, if you live in a region with low rates of insurance coverage, it's highly unlikely that you have a Level I trauma center nearby, since no hospital would invest in setting one up if most of their patients will be unable to pay. Which means if you have a car accident, you're just as screwed as someone without health insurance.
IMHO, this is an overlooked angle that universal healthcare advocates should stress to people who think universal coverage doesn't provide any benefit to people who already have insurance.
Hi WX! To which I would add: the quality of the equipment in hospitals is outdated…MRI machines, staffing ratios, traiining, etc. Those patients who are sophisticated and have better health insurance will seek quality care even if they have to leave their area, resulting in the local hospitals population having a higher indigent census. The list is like dominoes….it just rolls on and on. Thanks for the study link. I'm looking forward to reading it.
I am one of those people with accumulated medical issues. Trumpcare will kill me by denying me access to my doctors and my medications because I won't be able to afford insurance and I won't be able to afford medical care and medications.. It will set back America 100 years in social development. I find it extremely frightening to observe Trump's behavior and think that Congress isn't alarmed by it. If Trump were truly working at the job, in my opinion, he wouldn't have any time to spend on Twitter.
Trackbacks
Leave a Reply
Three Misunderstood Things
This week: the anti-gay baker, why the Senate can't move on, and whether raising the minimum wage kills jobs.
I. The Masterpiece Cakeshop case (which the Supreme Court will hear in the fall).
What's misunderstood about it: People think it has free-speech implications.
What more people should know: The baker objected to the whole idea of making a wedding cake for two men, and cut off the conversation before the design of the cake was ever discussed. That makes it a discrimination case, not a freedom-of-speech case.
*
Defenders of Masterpiece Cakeshop owner Jack Phillips frequently portray him as a martyr not just to so-called "traditional marriage", but to the freedom of tradespeople not to say things they object to. For example, one conservative Christian tried to demonstrate a double standard like this:
Marjorie Silva, owner of Azucar Bakery in Denver, said she told the man, Bill Jack of the Denver suburb of Castle Rock, that she wouldn't fill his order last March for two cakes in the shape of the Bible, to be decorated with phrases like "God hates gays" and an image of two men holding hands with an "X" on top.

Is this cake gay or straight?
But the Colorado Civil Rights Commission ruled against Jack, because the two cases are very different: Silva objected to the message Jack wanted on the cake, not to anything about Jack himself or the situation in which the cake would be served. If the government had demanded that Silva make that cake, it would have been an example of forced speech, which there is already a long legal history against.
Do conservatives also have a right to refuse forced speech? Yes. A Kentucky court recently ruled in favor of a print-shop that refused to make t-shirts for a gay-pride festival.
So liberals must have howled in rage, right? Not me, and not philosopher John Corvino, who defended the Kentucky decision on the liberal news site Slate:
the print shop owners are not merely being asked to provide something that they normally sell (T-shirts; cakes), but also to write a message that they reject. We should defend their right to refuse on free-speech grounds, even while we support anti-discrimination laws as applied to cases like Masterpiece Cakeshop. … Free speech includes the freedom to express wrong and even morally repugnant beliefs; it also includes the freedom for the rest of us not to assist with such expression.
The reason the baker has lost at every stage so far — the administrative court and state appeals court ruled against him, and the Colorado Supreme Court refused to hear his appeal, letting the lower court ruling stand — is that he wasn't objecting to putting some particular message or symbol on the cake, like a marriage-equality slogan or a rainbow flag. For all he knew when he refused, the men might have wanted a cake identical to one he had already made for some opposite-sex couple. In short, he objected to them, not to the cake they wanted.
Corvino explains:
One might object that Masterpiece Cakeshop is similar: "Same-sex wedding cakes" are simply not something they sell. But wedding cakes are not differentiated that way; a "gay wedding cake" is not a thing. Same-sex wedding cakes are generally chosen from the same catalogs as "straight" wedding cakes, with the same options for designs, frosting, fillings and so forth. It might be different if Masterpiece had said "We won't provide a cake with two brides or two grooms on top; we don't sell those to anyone." But what they said, in fact, was that they wouldn't sell any cakes for same-sex weddings. That's sexual orientation discrimination.
II. Mitch McConnell's agenda.
What's misunderstand about it: If the Senate is stuck on its ObamaCare replacement, why can't it move on to the next items on the Republican agenda: tax reform and the budget?
What more people should know: McConnell is trying to exploit a loophole in Senate rules. As soon as a new budget resolution passes, his ability to pass both TrumpCare and tax reform goes away — unless he changes the proposals to get Democratic votes.
*
During the Obama years, we often heard that "it takes 60 votes to get anything done in the Senate", as if filibusters that can only be broken with 60-vote cloture motions were in the Constitution somewhere, and the minority party had always filibustered everything. (That's why even the weakest gun-control bills failed, despite 54-46 votes in their favor.) But the Senate recognized a long time ago that budgets have to get passed somehow, and so the Budget Control Act of 1974 established an arcane process called "reconciliation" that circumvents the filibuster in very limited circumstances.
That's how the Senate's 52 Republicans can hope to pass bills without talking to the Democrats at all. But there's a problem: Reconciliation is a once-a-year silver bullet. Fox Business explains:
Reconciliation allows Congress to consider just three items per fiscal year, whether they pertain to one bill or multiple. Those items are spending, revenue and debt limit. Since the GOP also wants to pass its tax reform agenda using reconciliation, it cannot statutorily do that under this budget blueprint because the two policy measures overlap.
And NPR elaborates:
The budget resolution for the current fiscal year dictates that any reconciliation measure must reduce the deficit, which the GOP's Obamacare repeal was designed to do. Republicans then could draft a new budget resolution for the upcoming fiscal year with easier deficit targets, allowing for more aggressive tax cuts.
Under the most commonly accepted interpretation of the reconciliation rules, as soon as Congress passes a budget resolution for Fiscal Year 2018 (which begins this October), the window for passing TrumpCare under the FY 2017 resolution closes. So the only way to get them both done before facing another election campaign is to do them in the right order: first TrumpCare, then a new budget resolution, then tax reform.
Otherwise, McConnell's options become less appealing: He can get rid of the filibuster completely, which several Republican senators don't support. He can scrap either TrumpCare or tax reform for the foreseeable future. Or he can start envisioning the kinds of proposals that might get eight Democratic votes, plus a few to make up for Republican defections.
III. The minimum wage.
What's misunderstood about it: Both supporters and critics of an much-higher minimum wage think they know what effect it will have on jobs.
What more people should understand: The effect of a minimum-wage increase on jobs is an empirical issue, not something you can deduce from first principles. And the data we have only covers small increases.
*
There is a certain kind of conservative who thinks he learned everything he needs to know about this issue in Econ 101: Every commodity, including unskilled labor, has a demand curve; if you raise its price, demand for it falls.
The right response to that analysis is maybe. Imagine that you own a shop with one machine, run by your sole employee. The machine produces some high-profit item. To make things simple, let's ignore counterfeiting laws and imagine that the machine prints money. Cheap paper and ink go in, $100 bills come out.
Obviously, you could afford to pay your employee a lot more than the $7.25-per-hour federal minimum wage. But you don't, because the machine is simple to operate and you could easily replace him, so he doesn't have any bargaining leverage.
Now what happens if the minimum wage goes up to $15? Do you fire your guy and shut the machine down? Do you abandon your plan to buy another machine and hire a second worker? No, of course not.
Admittedly, that's an extreme example, but it points out the right issues: Whether an increase in the minimum wage causes you to employ fewer people depends on how much you're making off those people's work. If you have a razor-thin profit margin, maybe a higher wage makes the whole operation unprofitable and you lay workers off. But if you could actually afford the higher wage, and the only reason you don't pay it already is that your workers lack bargaining leverage, then you don't.
In fact, if a minimum-wage increase gives your customers more money to spend on whatever you make, then you might have to hire more people to meet the demand.
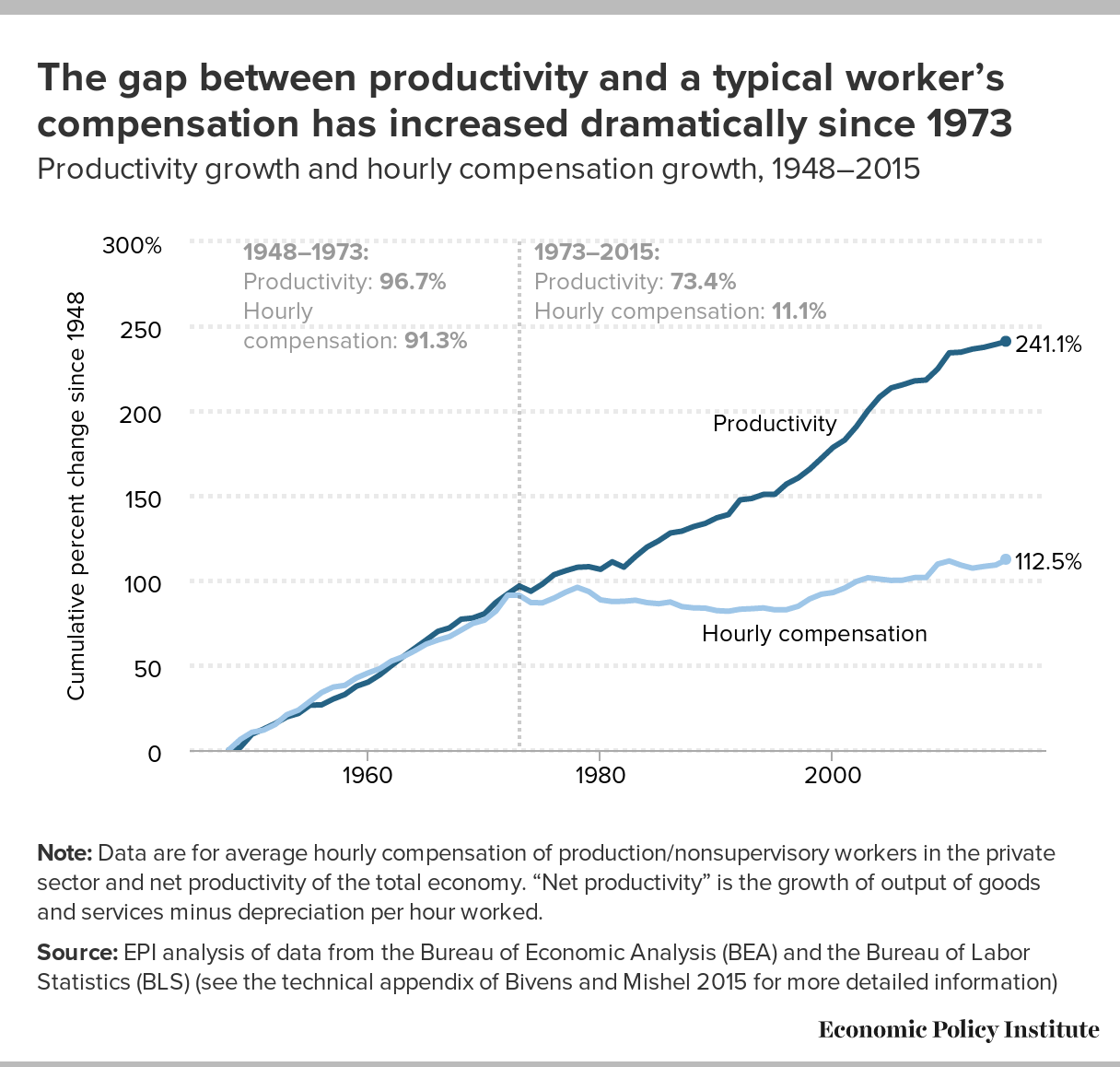
Which situation is more typical? One reason to think the second situation is, is that sometime in the 1970s wages stopped tracking productivity: Workers have been producing more, but not getting comparable pay raises, presumably because they lack the bargaining power to demand them.
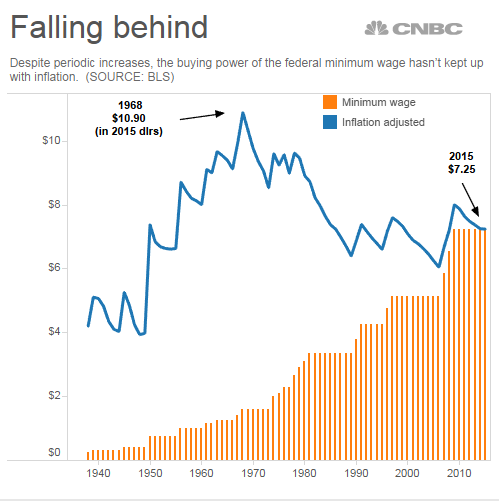
During the same era, the minimum wage has not kept pace with inflation. An increase to around $11 would just get it back to where it was in 1968. If it wasn't causing massive unemployment then, why would it now?
 Supporters of a higher minimum wage also point to studies of past increases, which don't show big job losses.
Supporters of a higher minimum wage also point to studies of past increases, which don't show big job losses.
But there's a problem on that side, too: Past hikes haven't been nearly as big as the proposal to go from $7.25 to $15. I was a minimum-wage worker myself in the 1970s when it increased from $1.60 to $1.80. I suspect my employer was not greatly inconvenienced. But larger increases might have a shock value that makes an employer say, "We can't afford all these workers."
That's why the new data coming in from Seattle is so important: Seattle was one of the first cities to adopt a much-higher minimum wage, so we're just beginning to see the results of that. The headlines on that initial study were that the higher wage is costing jobs, but that early conclusion is still debatable.
So in spite of my own preference for a higher minimum wage, I find myself in agreement with minimum-wage skeptic economist Adam Ozimek: This is an empirical question, and both sides should maintain more humility until we see more definitive data.
Comments
A further question about your example of the machine that prints money and minimum wage is:
At what point is it more profitable for the owner to buy a machine that doesn't need a worker to print the money? Will increasing the minimum wage lead us closer to that problem of employment?
If so, should we have a basic income? Should minimum wage be a living wage for those that can work and we'll write off automation until some later date (which may be sooner than we'd like)?
I'm all for increasing the minimum wage to keep up with inflation, but I worry that we will see a point in the not too distant future where the wage to employ someone is high enough that owners may just buy a machine that would do the job anyway. Then we need to decide what to do with the people who are now unemployed and can't get a job (lack of skills? inability to move? etc.).
Those are good questions, and also come up on this blog from time to time. Ultimately, I think we will need a basic income, but we'll have to change a lot of our social assumptions and habits to make that work.
I agree with you. I think we need a basic income, but I think it seems more unlikely than ever with our current political climate.
We own a bike shop and the minimum wage in our California city went from $10.50 to $12 on July 1, and is going to $15 by Jan 2019; voter approved. With a ~30% GPM, that's a big increase. I hope not to have to let anyone go because I would really like to pay as well as I can, but those are scary numbers.
Since every other bike shop is subject to the same wage regulations, wouldn't all of you just raise prices to cover the increase?
Have you looked into improving the Earned Income Tax Credit as alternative to major increases into the Minimum Wage? It's politically tougher because it increases government spending. But, it strikes me as a more rational and fair system.
I'm aware of debate over the two ideas, but I can't say I've really looked into it.
The other complicating factor in determining the effect of minimum wage increases is how it will affect jobs further "up the scale" as it were. For example, I know of a call center in a rural area which pays $11 an hour, because while they are low wage they don't want to be minimum wage. If minimum wage is raised to $15/hour they will have to raise their pay, but how much? If they increase only to $15 then they are minimum wage employers, but how much more can they increase it before it hurts their bottom line.
Or, since all of their competitors will be subject to the same regulations, they can just raise the price they charge customers to cover the increase.
I have a friend who owns a rental business (tables, chairs, event tents, bounce houses, large power tools, etc.) and he also pays a little over minimum wage for the sake of attracting and keeping unskilled but reliable workers. I made the same point about his competitors also having to increase wages and that they would all increase prices to compensate. My friend thinks the higher prices will result in people renting less stuff and less often. I think he's probably overestimating how much less, but like the article says, this is an empirical question. It will largely depend on things like whether families are already maxing out their backyard graduation party budgets, or how badly a contractor wants to avoid storage and maintenance for his own jackhammer vs periodically renting one. These are very concrete factors, not theoretical at all.
I would think an economist would be able to study the industry and answer that question. But this brings up another point – is a national, across-the-board minimum wage, like what we have now, only higher, the correct approach? $15 in rural Mississippi is pretty good, but it's starvation wages in Manhattan or San Francisco. A better solution would be a locally appropriate minimum wage to account for these regional differences, and given your friend's observations, maybe an industry or occupation-specific one as well, similar to what already exists under the Davis-Bacon or Service Contract Acts for federal construction projects and services.
Also, making $15 per hour won't help much if you're only working 20 hours per week. A true minimum wage that guaranteed a basic standard of living would be an annual rate, not an hourly one.
Nice format and content.
Also really like the "more light, not heat" tone.It feels good to write this way. I see this format as pushing me back towards roots of the Weekly Sift.
I'm not sure where you might want folks to make suggestions for this column. I'd like to see the term "job creator" discussed. Another one is the idea of government control — e.g., does "government" paying for Medicare and other health care equal control (versus regulations, say, on what an insurance policy must cover, mandatory disclosure, etc.). A third is the idea of a "market" as in let the "market" solve the problem. If one looks at the components of a "perfect" market in micro-economic terms, there are precious few "markets" out there. A fourth is the idea of an economic stimulus (think Keynesian and could be connected to the job creator discussion). A fifth is government, especially Federal, deficit and its purpose which could also be part of number four. I'll stop there. I like this format as I think there are so many misunderstood concepts and terms out there.
One of the daunting aspects of picturing this as a regular feature is whether I can come up with three good topics week after week. I appreciate suggestions, and the comment thread is a good place for them. Thanks.
An issue I think a lot of people on both sides are getting wrong is where sexism/racism/etc. intersect with statistical facts about demographics. For example, the average scores on certain quantitative/mathy standardized tests are a little bit higher for men than for women. How does that relate to the fact that my industry, software engineering, has a 10:1 ratio of men to women? Why is it still wrong to discriminate against female software engineers despite these statistics? There are good liberal answers to these questions, and then there are very bad liberal answers, (and VERY bad conservative answers,) and a lot of the confusion comes down to people not understanding what statistics and averages really mean.
That does sound like a good thing to cover. I'll need to do some background reading, so don't expect to see it quickly.
If there aren't three good topics a week, maybe it doesn't need to be every week. Maybe it's frequency should be "whenever there are good topics to cover"


No comments:
Post a Comment